OBSTETRICS -by Dr.V.VIBINRAJAN
1. OBSTETRIC-HAEMORRHAGE
Any kind of Heavy bleeding ( pregnancy) in a parturient during pregnancy, child birth, or in the postpartum period from vagina

TWO TYPES
ANTEPARTUM HAEMORRHAGE - Any cause of bleeding from genital tract after 28 week of pregnancy
POSTPARTUM HAEMMORHAGE - Any cause of bleeding from genital tract after delivery MCC of MMR in INDIA
POSTPARTUM HAEMMORHAGE (PPH):
- more than 500ml blood loss in normal delivery
- more than 1000ml blood loss in Cesaerian delivery
- Mild PPH - b/w 500ml to 1000ml blood loss
- MODERATE PPH - b/w 1000ml to 2000ml blood loss
- SEVERE PPH - more than 2000ml blood loss
- MASSIVE OBSTETRIC HAEMMORHAGE - more than 1500ml blood loss or loss of haemoglobin > 4gm % is PPH
- Any cause of bleeding from genital tract that reduce haemoglobin by 1gm % is PPH
PRIMARY PPH: heavy bleeding with in 1st 24 hrs of delivery mc in 1st 1hr
SECONDARY PPH: heavy bleeding after 24hrs of delivery uptill 12 weeks

PREVENTION OF PPH:

 - 90mu g/kg in 3 to 5 minutes IV infusion
- 90mu g/kg in 3 to 5 minutes IV infusion
HOW TO MANAGE PPH DURING DELIVERY?
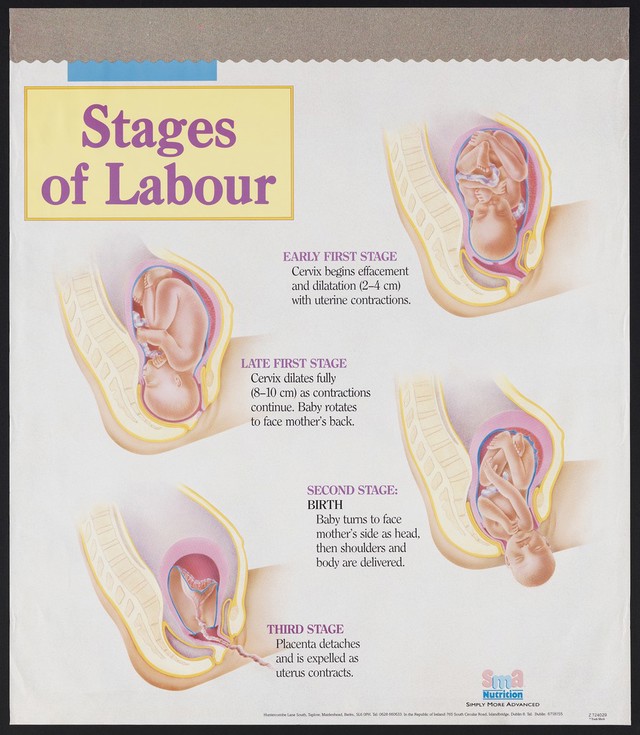
STAGES OF LABOUR

MANAGEMENT OF PPH ON 3RD STAGE OF LABOUR
1.Controlled cord traction and abdominal counter traction
2. uterine massage
3. administering OXYTOCIN

1.TONE - atonic uterus (contributes 80% of PPH)
causes due to
- Over distention of UTERUS(large uterus) - twins, big baby , increased amniotic fluid
- malnutrtition and anaemia
- antepartum haemorrhage
- infections- PROM, Chorioamnionitis
3.TISSUES : retained placental tissues, invasive placenta
retained placental tissues causes SECONDARY PPH
4.THROMBIN DEFICIENCY:
abnormal coagulation due to deficiency of
- VON WILLEBRANDS DISEASE - hereditary blood-clotting disorder due to deficiency of von willebrand factor
- ITP (idiopathic thrombocytic purpura)
PREVENTION OF PPH:
-prophylactic IM/IV OXYTOCIN ( DOC in PPH)
- conduct delivery properly especially at 3rd stage of labour
TREATMENT :
- IV OXYTOCIN (10-20 units drip) ( DOC )
- IV METHYL ERGOMETRINE 0.2mg (peak action at 90 sec)
Mechanism of action : contract uterus ms and increase uterine ms tone
Contraindications:
- Abdominal pain
- seizures
- cardiac diseases
- pregnancy induced hypertension
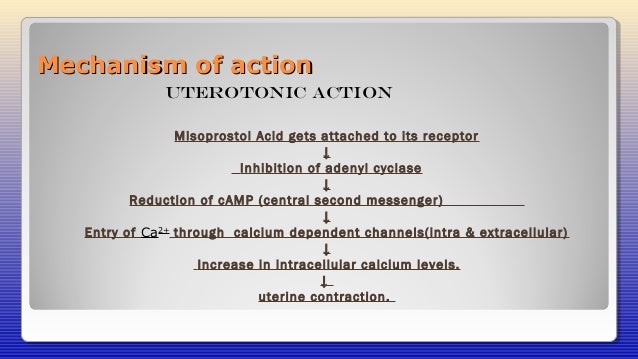
- T. MISOPROSTOL (PGE1) - 1000 mu g per RECTUM
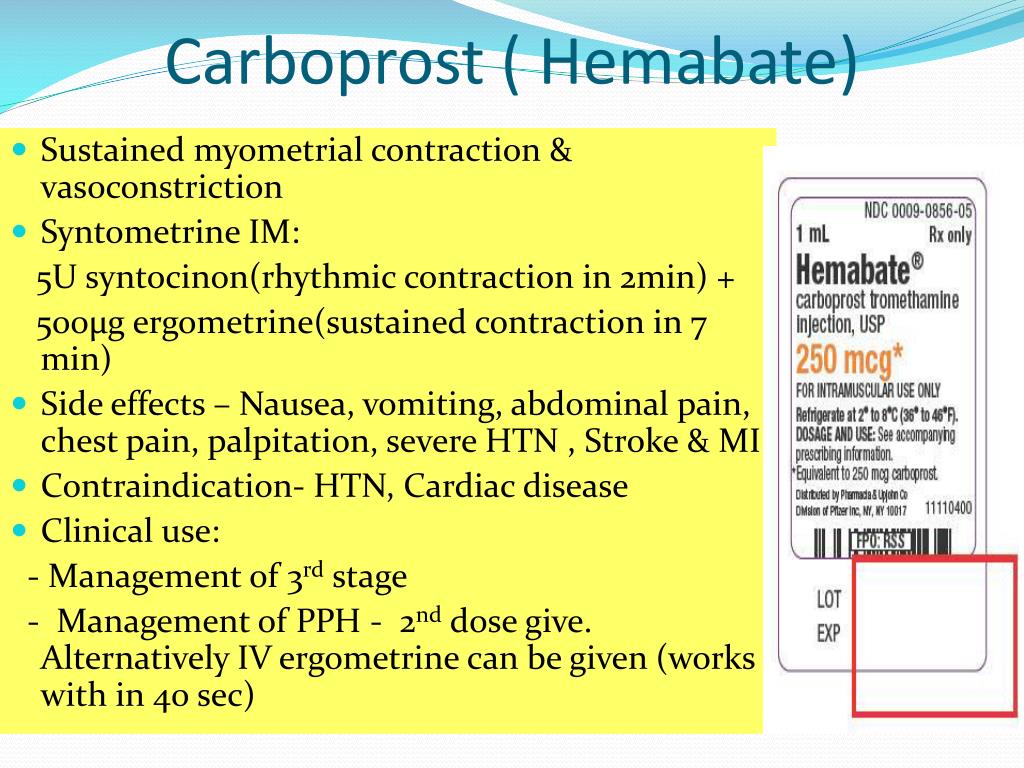
- CARBOPROST (PGF2alpha)
- not IV causes sudden HYPERTENSION
- RECOMBINANT ACTIVATED FACTOR 7
- FIBRINOGEN
- CRYOPRECIPITATE (3ml/kg) : 10 times > FFP(30ml/kg)
give 10 units of cryoprecipitate or 1litre of FFP
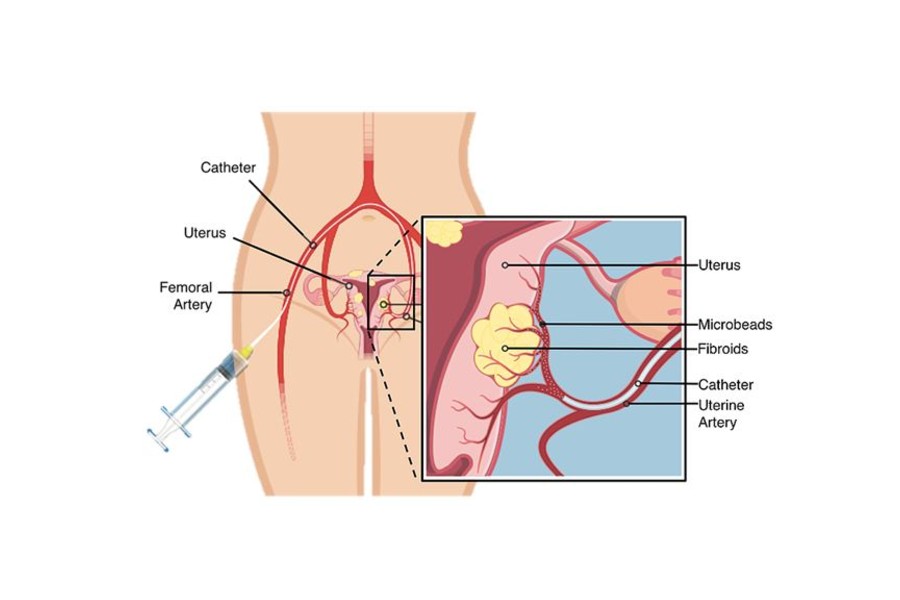
- UTERINE ARTERY EMBOLIZATION
- prophylaxis for PLACENTA PREVIA, PLACENTA ACCRETA

https://fibroidspecialistuae.com/image/uterine-artery-embolization.jpg
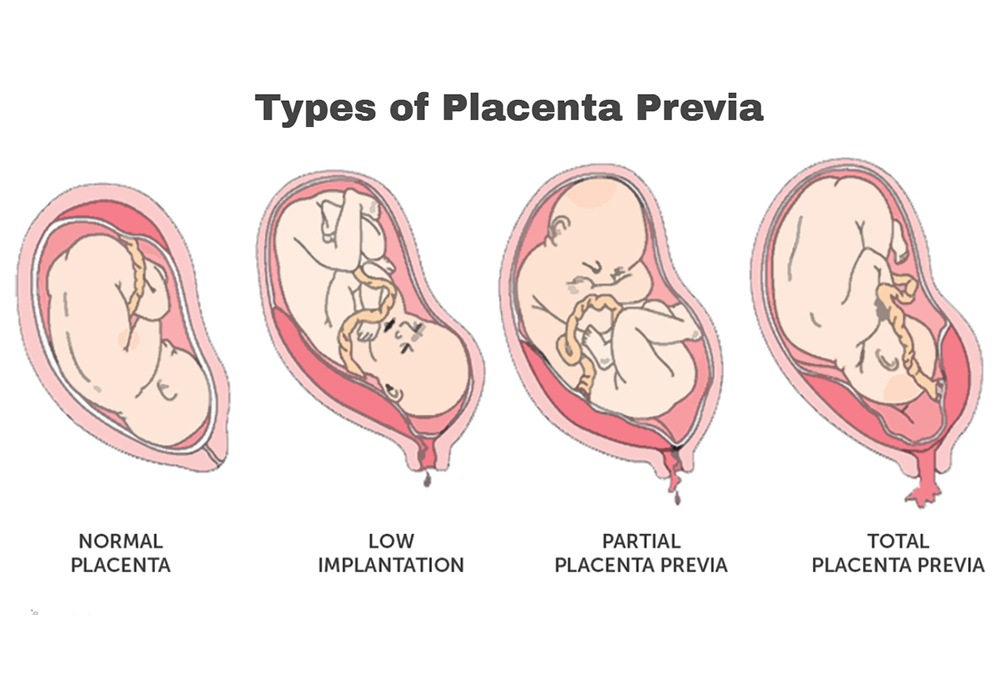
PLACENTA PREVIA- placenta grows in the lowest part of the womb (uterus) and covers all or part of the opening to the cervix.

PLACENTA ACCRETA

- INTRAVASCULAR AORTIC BALLOON COMPRESSION - prophylactic
- BALLOON TAMPONADE
- Bakri balloon
- Sengstaken tube
- Folleys catheter
- condoms

condom catheter - filled to 500 mL of fluid the condom catheter has no drainage tip.
latex and silicone Foley - each contains 30 mL of fluid.
Sengstaken - gastric balloon filled to 300 mL.
BT-Cath's drainage tip - flush with the end of the balloon; here it is filled to 500 mL of fluid.
Bakri balloon - filled to 500 mL.
ebb - filled to 750 mL in the uterine balloon .The ebb's drainage tip protrudes from the end of the balloon initially, but as the balloon fills, it no longer protrudes.
- SURGICAL METHODS


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Nice brief explanation
ReplyDelete